Nitazenes - What This New drug Means For British Policing
Synthetic opioids have landed in the UK. What nitazenes are, why they are more dangerous than the heroin they are displacing, and the strategic, tactical and operational picture for policing.
Nathan Tracey
Audio edition
≈ 21 min · narrated
Synthetic opioids are no longer a problem we’re watching arrive from across the Atlantic. They’ve landed. The National Crime Agency now links nitazenes to roughly 1,000 deaths in the UK since they appeared at scale in June 2023, a figure its Director General has called “extraordinary”.1 For an audience of senior leaders and policymakers, that single sentence reframes the question. This isn’t horizon-scanning. It’s an operational reality that most forces are under-resourced to detect, let alone respond to.
This piece sets out what nitazenes are, where they came from, why they’re more dangerous than the heroin they’re displacing, and what the strategic, tactical and operational picture looks like for British policing. I’ve tried to separate what the evidence clearly supports from what’s contested or assessed, because some of the loudest claims about these drugs — particularly around officer safety — don’t survive contact with the toxicology.
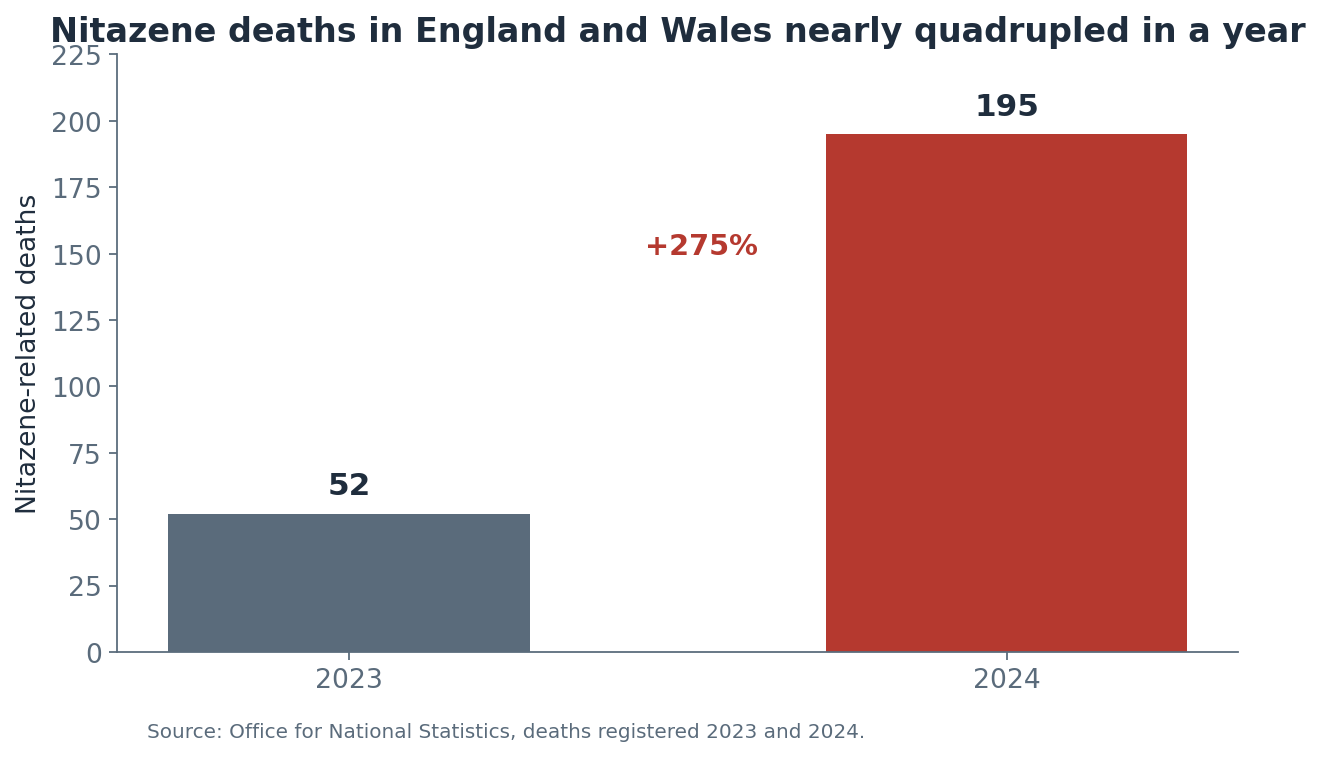 Nitazene deaths in England and Wales rose nearly fourfold in a single year. Source: ONS.
Nitazene deaths in England and Wales rose nearly fourfold in a single year. Source: ONS.
A 1950s laboratory accident, sixty years dormant
Nitazenes aren’t new chemistry. They’re benzimidazole opioids, first synthesised by the Swiss pharmaceutical firm CIBA in the 1950s as candidate painkillers. The problem was obvious almost immediately: they were far too potent, with a risk of fatal respiratory depression that made them unviable as medicines. They were never marketed.2 For roughly six decades they sat in the chemical literature, a footnote.
What changed wasn’t the science. It was the economics of supply. Nitazenes are fully synthetic, which means no poppy fields, no growing season, no geography. They can be made in a laboratory anywhere, from precursor chemicals that are often uncontrolled, and shipped in quantities small enough to defeat traditional interdiction. A package of a few grams can represent thousands of street doses.3 That combination — cheap, potent, easy to conceal, easy to manufacture — is exactly what a disrupted opioid market rewards.
And the market has been disrupted.
The Afghan supply shock
To understand why nitazenes have surfaced now, you have to look at Afghanistan. For decades it supplied the overwhelming majority of Europe’s heroin — around 95% of UK street heroin originated there. In April 2022 the Taliban announced a comprehensive ban on opium cultivation, and unlike the short-lived 2000–01 ban, this one has held. Poppy cultivation in Afghanistan collapsed by around 95%, with satellite imagery showing Helmand province down by over 99% in a single year.4
The effect on UK supply is now measurable. In the year to March 2024, the quantity of heroin seized in the UK fell by 54%, from 950kg to 441kg — the lowest figure since 1989. Wholesale heroin prices have risen from roughly £16,000 per kilo before the pandemic to around £26,000. The NCA assesses the ban has created market “uncertainty”.5
Here’s the strategic logic, and it’s worth stating plainly. The UK has the largest heroin market in Europe, with an estimated 300,000 users in England alone.5 If the heroin supply tightens, that demand doesn’t evaporate. It gets met by something else. Organised crime groups already controlling distribution networks have every incentive to plug the shortfall with synthetics they can manufacture themselves at over 99% lower raw-material cost.6 North America’s experience suggests that once synthetic opioids establish themselves in a market, you cannot put the genie back in the bottle — even if heroin supply later recovers.7
So the question facing UK policy isn’t whether to prevent a synthetic opioid transition. It’s whether we’re prepared for one that may already be underway.
Why these are not just stronger heroin
The instinct is to treat nitazenes as heroin with the dial turned up. That undersells the problem in three specific ways.
First, the potency. The most common nitazene is estimated at 250 to 900 times stronger than morphine; the most potent compounds run to several thousand times.8 Commonly cited figures put nitazenes at up to 500 times the strength of street heroin.2 The practical consequence is that the gap between a dose that gets someone high and a dose that kills them becomes vanishingly small. With heroin, that margin exists. With nitazenes, a tiny error in measurement — and these are being mixed by criminals, not pharmacists — is fatal.
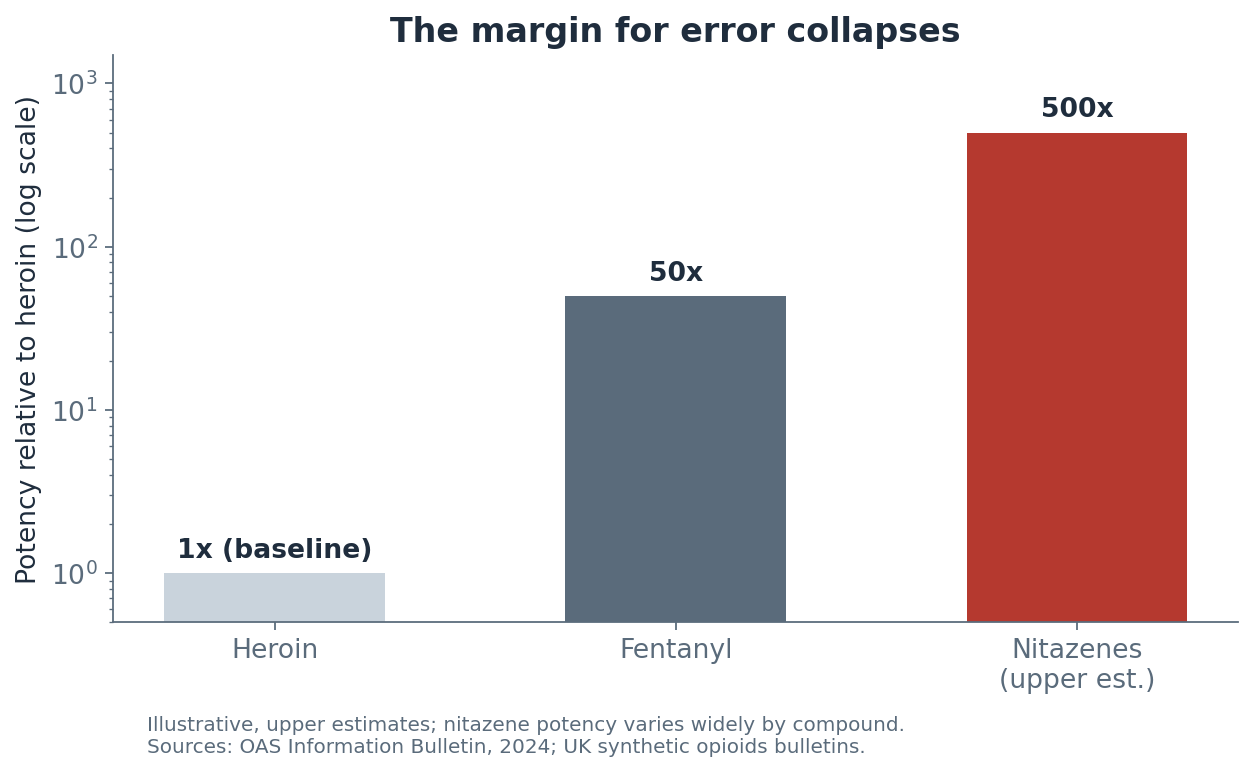 Relative potency, upper estimates, on a log scale. Nitazene potency varies widely by compound. Sources: OAS, 2024; UK synthetic opioids bulletins.
Relative potency, upper estimates, on a log scale. Nitazene potency varies widely by compound. Sources: OAS, 2024; UK synthetic opioids bulletins.
Second, the unpredictability. There are more than twenty distinct nitazene compounds in circulation, and the dominant one keeps changing. Twelve different forms have been detected in UK deaths.9 This matters because there’s no stable “dose” to learn. A user who survived last week’s batch has no reliable basis for judging this week’s.
Third, and most important for understanding the death toll: people often don’t know they’re taking them. Nitazenes have been detected adulterating heroin, but also cocaine, ketamine, synthetic cannabinoids (“spice”), and — critically — counterfeit prescription medicines. WEDINOS analysis has found them in substances sold as diazepam, oxycodone and Xanax.10 This is the dimension that breaks the traditional model of who’s at risk.
The counterfeit medicines problem changes the victim profile
Most opioid harm-reduction infrastructure is built around a known population: people who use heroin, who are in contact with treatment services, who can be reached with naloxone and messaging. The counterfeit pill route bypasses all of that.
Consider the NCA case of Robert Poleszak, a dark-web vendor who admitted supplying isotonitazene in 2026 (he is due to be sentenced in July 2026). He advertised oxycodone — a legitimate, recognisable painkiller — at up to 200 pills per transaction. The pills contained isotonitazene. He made more than 100 sales, with customer reviews noting that buyers had overdosed and ended up in hospital, and his supply was linked to the death of a drug user in Cornwall.11 The people buying those pills weren’t necessarily heroin users. They were people who thought they were buying a known pharmaceutical.
This is the opioid-naïve victim: someone with no tolerance, no naloxone in the house, no reason to think they’re at risk, and people around them who have no idea what they’ve taken when they stop breathing.12 A student buying what they believe is Xanax for anxiety. Someone buying oxycodone for pain because they can’t get a prescription. The death looks like a sudden collapse with no obvious cause, which is part of why these cases are so easy to miss.
The symptoms, and what they demand of a response
Clinically, nitazene toxicity presents like other opioid overdose: the classic triad of pinpoint pupils, depressed consciousness, and — the thing that kills — severe respiratory depression. The cause of death in overdose is the suppression of the drive to breathe, mediated through the μ-opioid receptor.13
Two features make the response harder than with heroin.
The respiratory depression is severe and prolonged. The fatal effects appear at much lower doses, and the depression can outlast the initial intervention.14
And naloxone, while it works, often isn’t enough on its own. This is the operationally critical point. Multiple or higher doses of naloxone are frequently required to reverse nitazene overdoses compared with heroin.13 The pharmacology behind this is becoming clearer: research published in 2025 found that nitazenes and fentanyls dissociate slowly from the μ-opioid receptor, which correlates with reduced sensitivity to naloxone reversal.15 Clinical reports describe patients needing prolonged naloxone infusions over several hours — well beyond the single-dose, short-observation model that current guidelines and lay naloxone kits assume.16
The implication for anyone carrying or supplying naloxone: one dose may buy time without solving the problem, and a patient who appears to recover can deteriorate again as the naloxone wears off faster than the opioid. Re-narcotisation is a real risk.17 Single-dose-and-walk-away is the wrong mental model.
Clearing up the officer-exposure question
There is a persistent belief, imported largely from US media, that officers can be poisoned simply by touching or being near these drugs at a scene. Senior leaders need the accurate version of this, because the inaccurate version has real costs.
The toxicology does not support the casual-contact overdose narrative. The American College of Medical Toxicology and the American Academy of Clinical Toxicology concluded that the risk of clinically significant exposure to emergency responders is extremely low. Fentanyl and its analogues are not volatile, so there’s no inhalation risk at a typical scene, and dermal absorption is very slow — estimates suggest it would take around fourteen minutes of both palms being covered in powder to absorb a therapeutic dose.18 The symptoms reported in the viral US “exposure” cases — racing heart, dizziness, shortness of breath, fainting — are not the symptoms of opioid toxicity. They are consistent with anxiety and panic, and toxicologists attribute them to the nocebo effect: people who believe they’ve been poisoned experiencing the symptoms they expect.19
This is not an argument for carelessness. Where officers might encounter airborne powder — a pill-pressing or manufacturing site, for instance — respiratory and eye protection are warranted, and gloves are sensible everywhere as routine practice.18 But the evidence is clear that the dramatic collapse-from-a-touch scenario is essentially a scientific impossibility, and overstating it carries a genuine operational cost. A US study found that fear of exposure leads responders to delay overdose intervention.20 An officer who hesitates to start rescue breathing or administer naloxone because they’re frightened of the powder is a worse outcome than the imagined risk they’re avoiding. Brief, evidence-based training measurably corrects the false belief: in one study, officers agreeing that touching fentanyl “could be deadly” fell from 80% to 39% after a short intervention.21 That’s a cheap, high-return piece of force-level work.
We are probably under-counting the dead
Every figure in this piece should be read with a caveat: the true death toll is almost certainly higher than recorded, and the surveillance gap is itself a strategic vulnerability.
The numbers we have are already alarming and inconsistent, which tells you something. ONS recorded 195 nitazene-related deaths in England and Wales in 2024, up from 52 in 2023 — close to a fourfold rise in a year.22 The NCA’s UK-wide figure for 2024 was higher, at 333.23 By March 2025, 285 deaths with nitazene detections had been reported to the National Programme on Substance Use Mortality, with the sharp increase landing in 2023.9 The discrepancy between sources reflects different counting methods and the fact that ONS data cannot reliably isolate synthetic opioid deaths at all.24
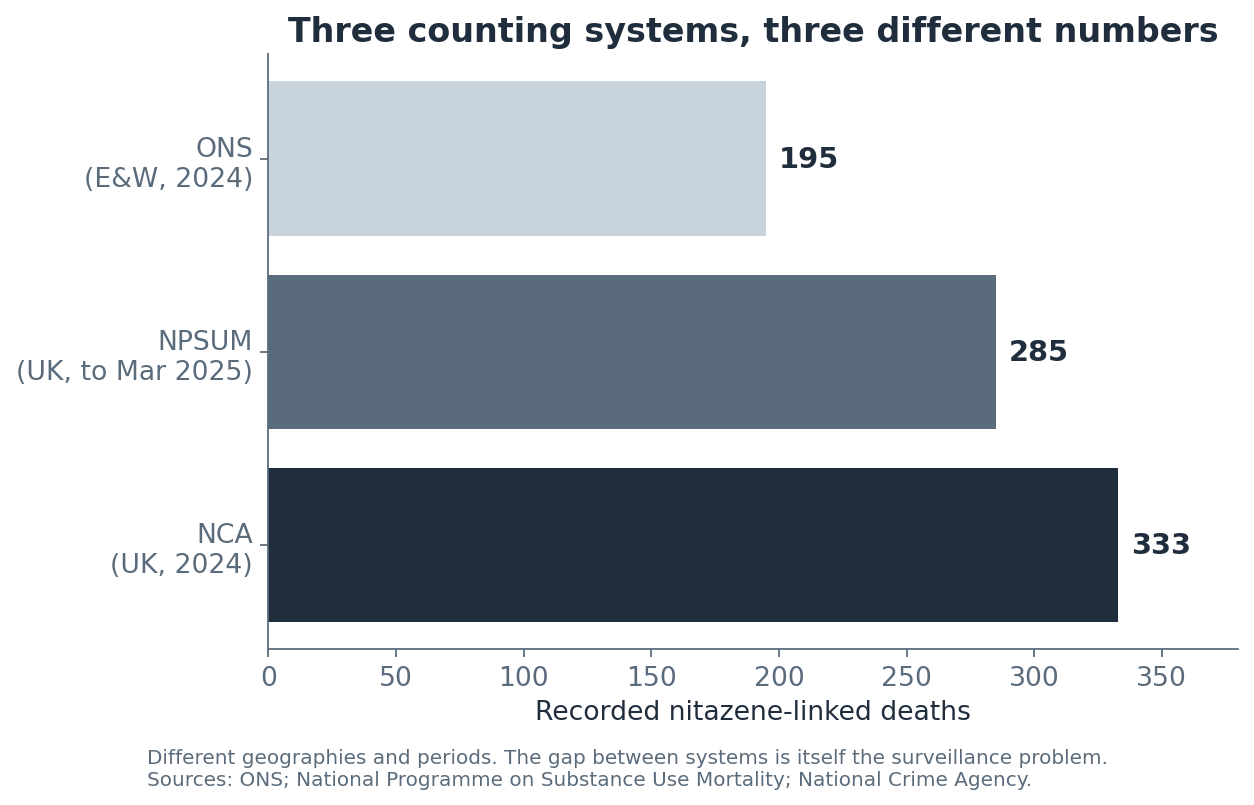 Three systems, three numbers. Different scopes and periods, but the gap between them is itself the surveillance problem. Sources: ONS; NPSUM; NCA.
Three systems, three numbers. Different scopes and periods, but the gap between them is itself the surveillance problem. Sources: ONS; NPSUM; NCA.
Then there’s the degradation problem. King’s College London research published in early 2026, combining a rat model with coronial data, found that nitazenes break down in post-mortem blood samples. The conclusion: we may be missing up to a third of the deaths nitazenes are involved in. As the lead researcher put it, public health responses are being designed and funded for roughly two-thirds of the real problem.23 If you’re allocating resource against the recorded figures, you’re under-resourcing by design.
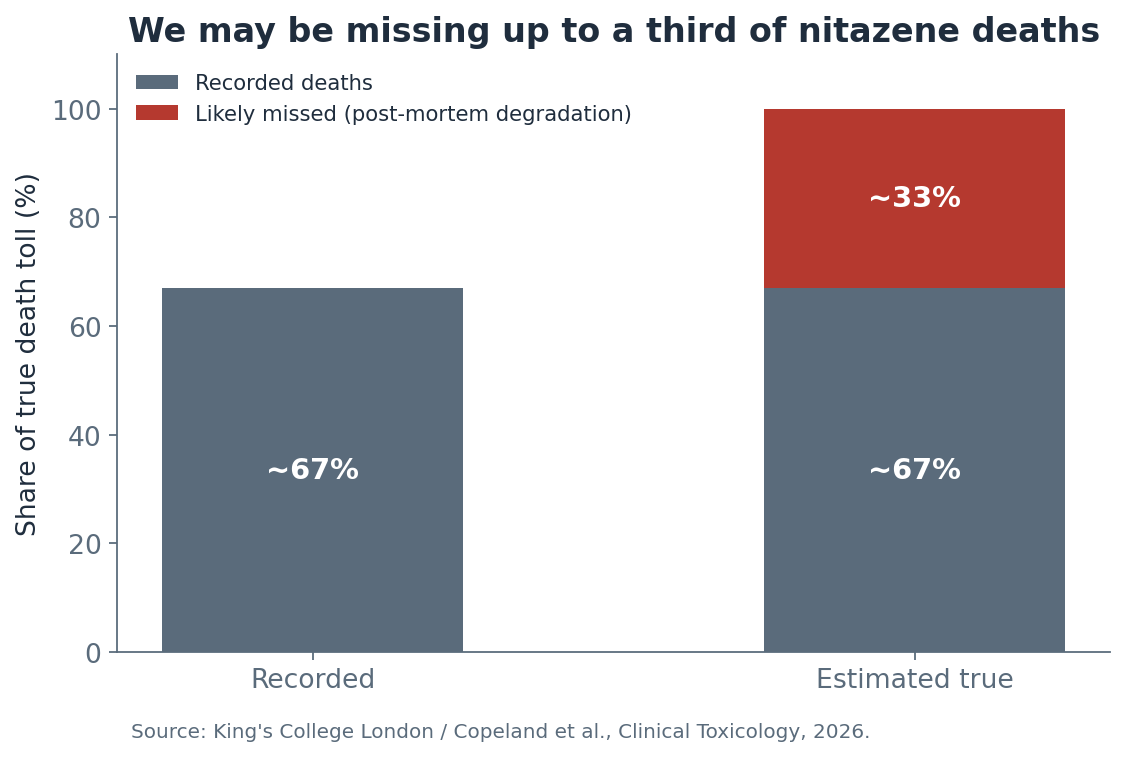 If recorded deaths represent only about two-thirds of the real toll, resource allocated against the official figures is short by a third before anyone starts. Source: King’s College London / Copeland et al., 2026.
If recorded deaths represent only about two-thirds of the real toll, resource allocated against the official figures is short by a third before anyone starts. Source: King’s College London / Copeland et al., 2026.
Detection is hard at every stage. Nitazenes are present in biological samples at very low concentrations, traditional drug screens miss them, and confirmation requires expensive, highly sensitive mass-spectrometry techniques that not every coroner or toxicology service routinely deploys.12 A force that isn’t actively looking for nitazenes will not find them — and will conclude, wrongly, that it doesn’t have a problem.
Strategic considerations for chief officers and policymakers
The central strategic judgement is this: treat nitazenes as a present threat requiring contingency planning, not a future one requiring monitoring. The supply-side conditions for a synthetic transition are in place, the deaths are already happening, and the recorded figures understate the scale.7
The national architecture already exists and forces should be plugged into it. The NCA’s Project HOUSEBUILDER has coordinated the law enforcement response since July 2023, alongside the HMG Synthetic Opioids Taskforce.25 Legislatively, the ground has shifted: in 2024 fifteen synthetic opioids including fourteen nitazenes were brought under the Misuse of Drugs Act as Class A, followed by a generic control based on chemical definition — a deliberate move to stop manufacturers staying ahead of the law by tweaking a molecule.26 That generic approach matters, because compound-by-compound scheduling is a game the chemists win.
Surveillance is where forces can most easily fall short, and where leadership attention pays off. OHID runs a drugs early warning system dashboard tracking synthetic opioid deaths and naloxone-involved ambulance call-outs in England.24 Public Health Scotland’s RADAR system issues rapid alerts.27 The strategic question for a chief officer is whether their force is actively contributing to and drawing from these systems, or passively assuming someone else is watching. Non-fatal overdose data, naloxone administration records and drug-checking results are the leading indicators of a cluster.28 A force that shares and monitors them can get ahead of one. A force that doesn’t will learn about a cluster from the body count.
Tactical considerations
At the tactical level, the West Midlands cluster of June–August 2023 is the closest thing we have to a template. Eighteen deaths and twenty-five non-fatal overdoses across the region triggered a multi-agency response, a National Patient Safety Alert from OHID, and — usefully — a structured College of Policing debrief afterwards.25 That debrief is worth reading by anyone designing a local response, because it treats a drug cluster as a “rising tide” emergency-preparedness event rather than business-as-usual drugs work.
Cluster response has to be genuinely multi-agency and pre-arranged. By the time a cluster is visible, there’s no time to build relationships from scratch. The local drug information system, public health, ambulance trusts, treatment providers and the police need a standing arrangement and a rehearsed playbook. Tabletop exercises run under the OHID preparedness framework have surfaced practical lessons — including that “nitazene” is poorly understood by the public compared with “fentanyl”, so harm-reduction messaging may need to use both terms.29
County lines intelligence is a tactical asset here. National preparedness exercises have noted that scene information from overdose clusters can be analysed through the county lines lens to identify supply routes and the people most at risk, and that Op PESTER-style tactics allow forces to push life-saving messaging directly to drug users connected to specific lines.29 The drugs intelligence picture and the harm-reduction picture are the same picture.
A word on communications, because it cuts both ways. The same exercises flagged that mishandled media or social media messaging can accidentally advertise a potent batch and increase demand.30 The instinct to warn the public has to be balanced against the risk of inadvertently marketing a product to the population most drawn to potency.
Operational considerations
On the ground, a few things follow directly from the evidence.
Naloxone provision should assume multiple doses and prolonged monitoring. Single-dose kits and the standard short-observation model are calibrated for heroin, not nitazenes. Officers, custody staff and anyone else carrying naloxone need to understand that apparent recovery can be temporary and that re-narcotisation is a live risk. The case for both intramuscular and intranasal formulations, and for higher-dose preparations, rests on this.31
Officer safety messaging should be proportionate and accurate. Routine gloves, sensible precautions, respiratory protection in the rare manufacturing-site scenario — yes. Fear-driven hesitation to deliver first aid — no. This is a training and culture issue that leadership can fix cheaply, and the cost of getting it wrong is measured in delayed interventions.20
Detection capability is a choice. If a force wants to know whether nitazenes are in its area, it has to look — through point-of-care test strips where appropriate, through ensuring its toxicology and coronial routes are sensitised to low-concentration synthetic opioids, and through feeding results into the local and national warning systems. Nitazene test strips are already referenced in some local preparedness plans.32
Custody is a specific pressure point. A detainee who has taken a counterfeit pill containing a nitazene may deteriorate hours after detention, beyond the window staff might expect for a heroin user, and may need repeated intervention. The opioid-naïve, polysubstance picture makes custody risk assessment harder, not easier.12
The verdict
Nitazenes are the predictable consequence of a supply shock meeting an unmet demand, and the predictable thing has happened. The reality — and I will resist dressing this up — is that British policing is responding to a crisis it is still partly blind to. The national structures are sound; the gap is local capability and, frankly, local willingness to go looking for a problem that’s easier not to find.
For senior leaders, three things matter above the rest. Get plugged into the surveillance systems and contribute to them, because the recorded figures understate the threat by design. Build the multi-agency cluster response before you need it, because you won’t have time afterwards. And fix the officer-safety messaging now, because the imported American panic costs lives at the exact moment an officer should be acting.
The question worth holding isn’t whether nitazenes will become a serious problem for UK policing. On the NCA’s own assessment, they already are. The question is whether forces will be able to see it clearly enough to respond — or whether we’ll keep designing our response around two-thirds of the dead.
Footnotes
-
Margaret Davies, “Synthetic opioid linked to 1,000 deaths across the UK in just two-and-a-half years,” The Independent, reporting Graeme Biggar (Director General, National Crime Agency) at the launch of the NCA National Strategic Assessment, 2026. ↩
-
“Potent synthetic opioid deaths on the rise,” Doctors.net.uk, February 2026; Local Government Association, “Local councils on the frontline: tackling nitazenes and drug-related deaths in England,” 2025 (origins as 1950s CIBA analgesics, never marketed; potency up to ~500x heroin). ↩ ↩2
-
National Crime Agency, “Drug supplier linked to nitazene deaths admits also making more than 5,000 indecent images of children,” 2026 (small volumes, fast-parcel smuggling, thousands of doses per few grams); Thermo Fisher / Identifying Threats, “Nitazenes: An Emerging Threat to Law Enforcement,” October 2025. ↩
-
BBC / David Mansfield satellite analysis and UNODC Afghanistan Opium Survey, summarised in “Rise in fentanyl and nitazene overdose deaths as Taliban enforces opium ban,” Substance Misuse Resources, February 2025; “Nitazenes’ Rise in the UK,” 2023 (~95% of UK street heroin sourced from Afghanistan). ↩
-
“There has never been a more dangerous time to take drugs: the rising global threat of nitazenes and synthetic opioids,” The Conversation / Policing Insight, 2025 (54% fall in UK heroin seizures to 441kg in year to March 2024, lowest since 1989; wholesale price rise; NCA “uncertainty” assessment; ~300,000 heroin users in England; largest heroin market in Europe). ↩ ↩2
-
P. Reuter et al., cited in “How to improve the surveillance of the Taliban ban’s impact on European drug markets,” International Journal of Drug Policy, 2024 (synthetic opioids can reduce wholesale raw-material costs by over 99%). ↩
-
Transform Drug Policy Foundation, “Taliban Opium Ban: What the future holds,” 2023; “How to improve the surveillance of the Taliban ban’s impact on European drug markets,” International Journal of Drug Policy, 2024 (post-2000 European precedent; irreversibility of synthetic transition; need for contingency planning). ↩ ↩2
-
Organization of American States, “Information Bulletin: The Emergence of Nitazenes in the Americas,” September 2024 (most common nitazene ISO ~250–900x morphine; most potent up to ~4,300x morphine). ↩
-
National Programme on Substance Use Mortality data to March 2025, reported in C. Copeland et al., “Is nitazene-related mortality underestimated?”, Clinical Toxicology, published online February 2026 (285 detections; twelve forms; clusters in 2021 and 2022, sharp rise in 2023). ↩ ↩2
-
WEDINOS analysis cited in “Afghanistan sees shift from opium to methamphetamine production,” Drink and Drugs News, 2023; Royal Borough of Greenwich, “Synthetic Opioids Bulletin,” March 2025 (detections in heroin, cocaine, spice, counterfeit benzodiazepines and oxycodone). ↩
-
National Crime Agency, R v Robert Poleszak press release, 2026 (oxycodone laced with isotonitazene; 100+ sales; customer reviews reporting overdoses; due for sentencing 17 July 2026). ↩
-
“Nitazenes: The Emergence of a Potent Synthetic Opioid Threat,” PMC (NCBI), 2025 (mis-sale as counterfeit medication; opioid-naïve users; analytical challenges; low sample concentrations requiring LC-MS). ↩ ↩2 ↩3
-
“Nitazenes: review of comparative pharmacology and antagonist action,” Clinical Toxicology, 2025 (clinical presentation; μ-opioid receptor mechanism; multiple/prolonged naloxone dosing in practice). ↩ ↩2
-
Royal Borough of Greenwich, “Synthetic Opioids Bulletin,” March 2025 (respiratory suppression; fatal effects at much lower doses). ↩
-
R. Alhosan et al., “Slow dissociation kinetics of fentanyls and nitazenes correlates with reduced sensitivity to naloxone reversal at the μ-opioid receptor,” British Journal of Pharmacology, 2024/25. ↩
-
“Nitazenes: review of comparative pharmacology and antagonist action,” Clinical Toxicology, 2025 (six of thirty patients required naloxone infusion over several hours, exceeding the one-hour observation in current guidelines). ↩
-
“Naloxone in Xylazine, Nitazenes, and Fentanyl Analogue Overdose,” Medical Toxicology, December 2025 (re-narcotisation risk; infusion triggers; short naloxone duration relative to opioid effect). ↩
-
American College of Medical Toxicology / American Academy of Clinical Toxicology, joint position statement on first-responder fentanyl exposure, 2017, and ACMT collaboration on “Fentanyl Safety Recommendations for First Responders” (risk of clinically significant exposure “extremely low”; non-volatile; slow dermal absorption; ~14 minutes with both palms covered; precautions for airborne-powder environments). ↩ ↩2
-
National Harm Reduction Coalition, “Myths and Misinformation About Law Enforcement and Fentanyl Exposure,” 2022; “Training to reduce emergency responders’ perceived overdose risk from contact with fentanyl,” PMC (NCBI) (symptoms consistent with panic, not opioid toxicity; nocebo effect). ↩
-
J. Beletsky et al., “Fentanyl panic goes viral: The spread of misinformation about overdose risk from casual contact with fentanyl,” International Journal of Drug Policy, 2020 (responders may delay overdose intervention to avoid perceived risk). ↩ ↩2
-
“Training to reduce emergency responders’ perceived overdose risk from contact with fentanyl: early evidence of success,” PMC (NCBI) (agreement that touching fentanyl “could be deadly” fell from 80% to 39% after a brief online training intervention). ↩
-
Office for National Statistics, deaths involving nitazenes, England and Wales, 2024, reported in “Synthetic opioid deaths almost quadruple as drug deaths hit record high in England and Wales,” ITV News, October 2025 (195 deaths in 2024, up from 52 in 2023). ↩
-
King’s College London, “UK’s growing synthetic opioid problem: Nitazene deaths could be underestimated by a third,” March 2026, reporting Copeland et al., Clinical Toxicology (NCA figure of 333 fatalities for 2024; post-mortem degradation; up to one-third undercount; “two-thirds of the real problem”). ↩ ↩2
-
Office for National Statistics, “Drug poisoning involving nitazenes and fentanyl” (FOI response) (ONS cannot isolate synthetic opioid deaths; OHID drugs early warning system dashboard covers England, including naloxone-involved ambulance call-outs). ↩ ↩2
-
Office for Health Improvement and Disparities, “Local preparedness for synthetic opioids in England,” GOV.UK, June 2025 (NCA Project HOUSEBUILDER from July 2023; HMG Synthetic Opioids Taskforce; West Midlands cluster — 18 deaths, 25 non-fatal overdoses; National Patient Safety Alert; College of Policing structured debrief). ↩ ↩2
-
House of Commons Library, “Debate on prevention of drug deaths,” Debate Pack CDP-2025-0071, March 2025 (Misuse of Drugs Act 1971 (Amendment) Order 2024 controlling 15 substances including 14 nitazenes as Class A; generic control via the No. 2 Order 2024). ↩
-
Public Health Scotland, “Rapid Action Drug Alerts and Response (RADAR) Alert: Nitazenes,” v2.0. ↩
-
Holland et al., “Nitazenes — heralding a second wave for the UK drug-related death crisis?”, The Lancet Public Health, 2024 (drug-checking and overdose-prevention services as harm-reduction and intelligence sources); OHID early warning system dashboard. ↩
-
Office for Health Improvement and Disparities, “Local preparedness for synthetic opioids in England,” GOV.UK, June 2025 (tabletop-exercise findings on public understanding of “nitazene” versus “fentanyl”; county lines intelligence and Op PESTER messaging tactics). ↩ ↩2
-
Greater Manchester Combined Authority, “Potent Synthetic Opioids (PSO) risk plan for Greater Manchester” (risk that mishandled media or social media messaging increases demand and overdose risk). ↩
-
Holland et al., “Nitazenes — heralding a second wave for the UK drug-related death crisis?”, The Lancet Public Health, 2024 (expansion of naloxone provision; both intramuscular and intranasal formulations). ↩
-
Office for Health Improvement and Disparities, “Local preparedness for synthetic opioids in England,” GOV.UK, June 2025 (nitazene point-of-care test strips referenced in local preparedness plans; test-strip data feeding local drug information systems). ↩